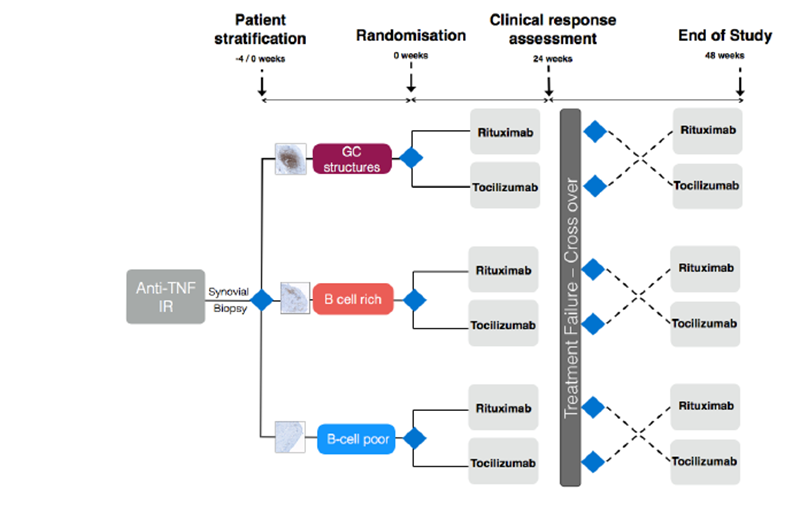
Current NICE guidelines recommend that patients who fail to respond to anti-TNF agents should be commenced on Rituximab, a monoclonal antibody against CD20 antigen expressed by B-cells. Other biologic agents include Tocilizumab, an inhibitor of interleukin 6(IL-6) which mediates inflammation within the joint. Current data suggests that the response to Rituximab therapy is variable, with only 60% reaching an ACR20 response at 6 months. (4)
We are a strong musculoskeletal unit and through our pathobiology of early arthritis (PEAC) cohort have pioneered minimally invasive ultrasound guided synovial biopsies in the UK. The use of this diagnostic tool will allow us to stratify responders / non-responders to Rituximab according to their synovial pathotype; more specifically to the absence or presence of B-cells within the joint lining. We have excellent links with other centres and will collaborate with the Barts Cancer Institute and Genome Centre at the William Harvey Research Institute in order to gain sight into disease response and relapse at the molecular and genomic level.
Our overall goals are to provide better clinical care through timely, stratified intervention with an appropriate choice of biologic, thus improving efficacy and reducing cost to the NHS.
Understanding the molecular basis of response and relapse will allow us to further understand the inflammatory process and ultimately open pathways into further therapies that will achieve and sustain disease remission.